
Why I still use CBT in therapy
Disclaimer: We want to affirm our commitment to neurodiversity and inclusive language practices. We utilize identity-first language, acknowledging the preferences of the community we serve. Therefore, you may notice us referring to individuals as "adhd people" rather than "people with adhd." This choice reflects our dedication to respecting the autonomy and identity of each individual. Studies have indicated that many within the autistic community prefer the term "autistic person," emphasizing the importance of recognizing and honoring diverse perspectives. Thank you for joining us on this journey of understanding and acceptance.
Welcome to a special blog post from our newest therapist, Alex McLaughlin! Alex is working with clients ranging from early childhood to adults in Minnesota, both virtually and in person in Edina! They currently have openings and would love to chat to see if they are a good fit for you!
CBT, otherwise called: cognitive behavioral therapy, has gotten a bad rap lately, and for good reason. People, and especially neurodivergent individuals, have been harmed by clinicians using CBT in ways that are invalidating, hurtful, culturally-unaware, and in situations where CBT is not relevant.
These experiences that folks have had are totally valid. I feel sad to know that folks have experienced harm, oppression, substandard or unethical therapy.
And if you’re someone that’s had enough bad experiences with CBT that you’re not interested in working with a therapist who incorporates it, I totally understand! On entertaining the idea of how CBT could be helpful, you get an instant sinking feeling in your gut, accompanied by David Rose’s voice saying, “hard pass,” then celebrate you tuning into your body, and close this blog post.
If on the other hand, you’re a wee bit curious to learn how it can be applied in relevant situations, with compassion, and oodles of validation, then continue reading. It may be helpful to read with the intention of approaching this post with curiosity, and desire to learn.
Let’s say that by the end of this, you’re still not on-board, I hear you and respect that! It's crucial to trust your instincts when choosing a therapist. and which modalities could meet your needs.
So, that said, let’s dive in!
What is CBT anyway!?
The American Psychological Association (APA, 2017) defines CBT:
“Cognitive behavioral therapy (CBT) is a form of psychological treatment that has been demonstrated to be effective for a range of problems including depression, anxiety disorders, alcohol and drug use problems, marital problems, eating disorders, and severe mental illness. Numerous research studies suggest that CBT leads to significant improvement in functioning and quality of life. In many studies, CBT has been demonstrated to be as effective as, or more effective than, other forms of psychological therapy or psychiatric medications” (2017).
CBT operates under a few principles:
Our thoughts, behaviors and emotions are all interconnected (see the CBT triangle below)
Mental health challenges can be based, in part, on unhelpful and/or untrue ways of thinking (i.e. “Everyone hates me.”)
Mental health challenges can come from, in part, by learned patterns of unhelpful behavior, that likely once served a survival or coping mechanism, however may now, cause other challenges as a result (i.e. everyone hates me, so I will shut down in social situations, or avoid them entirely, because that reduces the likelihood that I’ll be hurt or rejected).
By exploring the relationship between the ways we interpret, perceive / think, and respond to those interpretations and thoughts, we may be able to improve our mental health and reduce suffering.
How has CBT been used by therapists in ways that are harmful?
When therapists mis-apply CBT, it can be harmful when:
It invalidates a person’s lived experience
Puts a person in harm’s way (i.e. by asking someone to change a behavior that is keeping them safe).
It is applied indiscriminately, by a therapist who lacks judgment or sensitivity in regards to determining when CBT may be appropriate and helpful.
When not frontloaded with validation, and without the belief that all behaviors serve a purpose.
It is not approached from a decolonial, trauma-informed lens (i.e. asking a person who is experiencing oppression to reconsider the thought, “there are systems that exist to oppress me.”)
A client with harm OCD is told to “change their thoughts.” Fun fact, Kyle, folks do not choose to have intrusive thoughts / obsessional doubts about st@bb{ing a loved one.
Unfortunately, there are likely a bunch more stories of ways in which therapists have used CBT that results in harm to clients.
So now that we’ve explored what CBT is, and how it can be used in ways that cause harm, let’s dive more into the CBT triangle.


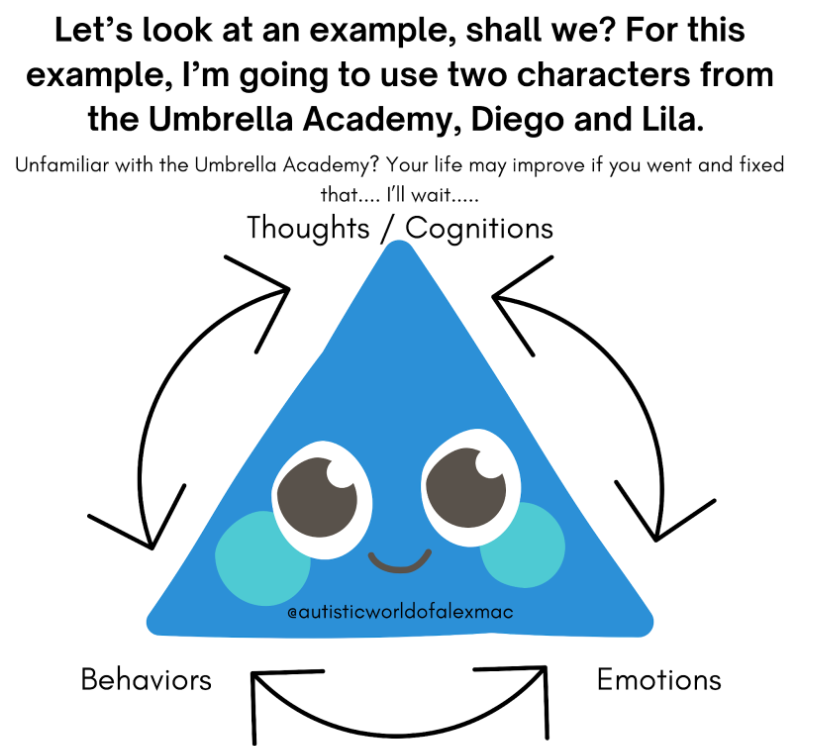




Now that you understand a bit more about the CBT triangle, let’s look at an example of how I might apply CBT in therapy.
Remember the principles of CBT mentioned earlier? Let’s explore some examples:
If a person has experienced bullying, rejection, and ridicule, time and time again; they may come to believe the thought, that “everyone hates me.” Believing this, as a result of their life experiences is COMPLETELY VALID. Who wouldn’t come to that conclusion!? That said, while they may have had mostly negative experiences in social situations, it is likely untrue that TRULY everyone they’ve ever met HATES them. There, afterall, nuance and gray in life. And believing this thought, may not be helpful to them, we’ll explore that a bit more with the next point.
So if someone believes the thought, “everyone hates me,” and have had life experiences where they were treated unkindly, in abusive ways, rejected, etc. they may shut down, and/or avoid social situations, all-together. This may currently serve, or have served a way for them to protect themselves. If shutting down and/or avoiding does not serve someone in ALL situations, and they have capacity to do, it could be helpful to explore the gray in the thought, and explore the potential negative consequences to shutting down and/or avoiding socializing (i.e. isolation, loneliness, anger, depression symptoms, increased anxiety, etc.). Because after all, we are, for the most part, social beings, and as a human species, need others for connection, and survival.
Also, as an aside, avoidance, while functional at times, can actually make anxiety worse (more on that later).
So let’s breakdown how I might approach a client in this scenario.
Let’s say a client says this thought a few times in therapy, and I’ve started to notice that it may be a pattern for them. We might compassionately explore if the thought is 1. True and 2. Helpful? If they say it’s true, and provide context, as to wy they think that. I will usually explore if there it is ABSOLUTELY true in all scenarios and situations. Then we might “look for the evidence” or “check the facts” on that. How do we know it’s true (i.e. has every single person in our lives that we’ve ever met told us these words)? Are we making assumptions, jumping to conclusions?
Then if we establish that there is some gray, next, we’ll explore if the thought is helpful? How does this thought serve them? Does it have any negative consequences?
Let’s say we land on; it can be true, but it’s not absolutely true; and discover together that thinking this way causes us to want to shut down out of protection.
I might celebrate with them that their body and brain are smart as heck and have kept them safe.
Then we might explore if it’s possible to reconsider their thoughts, maybe we first land on a thought that is more neutral, such as:
Most people hate me, there are some people who seem to tolerate me.
It seems most people hate me, though it’s not 100% true, there is that barista that remembers my name, my order and is usually friendly to me.
If they’re open to take it a step further, we might explore other thoughts to reconsider, a few examples may be:
I have had several negative experiences in social situations. Those are completely valid. There are some people who don’t seem to hate me from the core of their being.
Some people can be mean, and I’ve experienced that first-hand. There are also some people who are kind, and compassionate. I choose to be open to the possibility that I can build connections with people that earn my trust, and vulnerability.
A note on CBT protocols
There are some approaches to CBT that are a more structured protocol. There are times and places to use more of a structured approach. Some of those being Exposure and Response Prevention (ERP) for obsessive compulsive disorder (OCD) and inference-based cognitive behavioral therapy (I-CBT).
When applying CBT outside of these structured protocols, it can be applied and used in ways that are more fluid. For example, it can be used at a session when the need for its use arises, and other modalities can be incorporated alongside CBT, as clinically relevant.
Closing thoughts
So, if you’ve made it this far, can you see how exploring the relationship between our thoughts, emotions and behaviors can make an impact on our mental health?
Are you unconvinced? That’s okay! I am glad you kept an open mind and honestly impressed you’ve made it this far!
Could I be wrong about CBT and it actually be something that is ALWAYS harmful? Absolutely! I am open to having my mind change as I learn and apply CBT in my practice. For now, I will continue to gather qualitative data about how life changing CBT can be both for me, and clients.
Are you wanting to learn more?
Such as what DBT (dialectical behavioral therapy) is, and how it incorporates CBT?
Or how CBT is the foundation of other therapeutic approaches that have proven to be effective at treating challenges such as:
Obsessive compulsive disorder (OCD)
Anxiety (including social anxiety)
Depression
Trauma
Then let us know what topic you’d like me to do a deeper dive into next!
Contact us to learn more about therapy or to schedule a session. We look forward to partnering with you!
A little about Alex (they/them): I’m an AuDHD, non-binary, queer, disabled, chronically ill, and multi-racial clinical social worker / therapist, with lived experience of OCD + other mental health conditions. I provide individual therapy for clients ages 6-45.
Footnotes:
1 This is a non-exhaustive list of the ways in which therapy, including the use of CBT has negative impacts on people.
2 David Rose is a character from the tv show that originally aired on Netflix called, “Schitt’s Creek” (which can now be streamed on Hulu, among other streaming services; this link is not sponsored)
3 There are likely more examples.
4 OCD stands for obsessive compulsive disorder. People who live with OCD have different content of their intrusive thoughts / obsessional doubt, sometimes referred to as “themes,” One theme of OCD is commonly referred to “harm OCD,” in which a person has intrusive thoughts / obsessional doubts about harming others and/or themselves, which is not consistent with who they are and their values in life.
5 Kyle is the male equivalent to Karen, which has been popularized by culture in reference to a white person, usually a female-presenting individual, who feels entitled and usually complains to managers. No hate to Kyles or Karens, there are Karens and Kyles that absolutely do not fit this profile.